How To Complete An Individual Progress Note From The Calendar
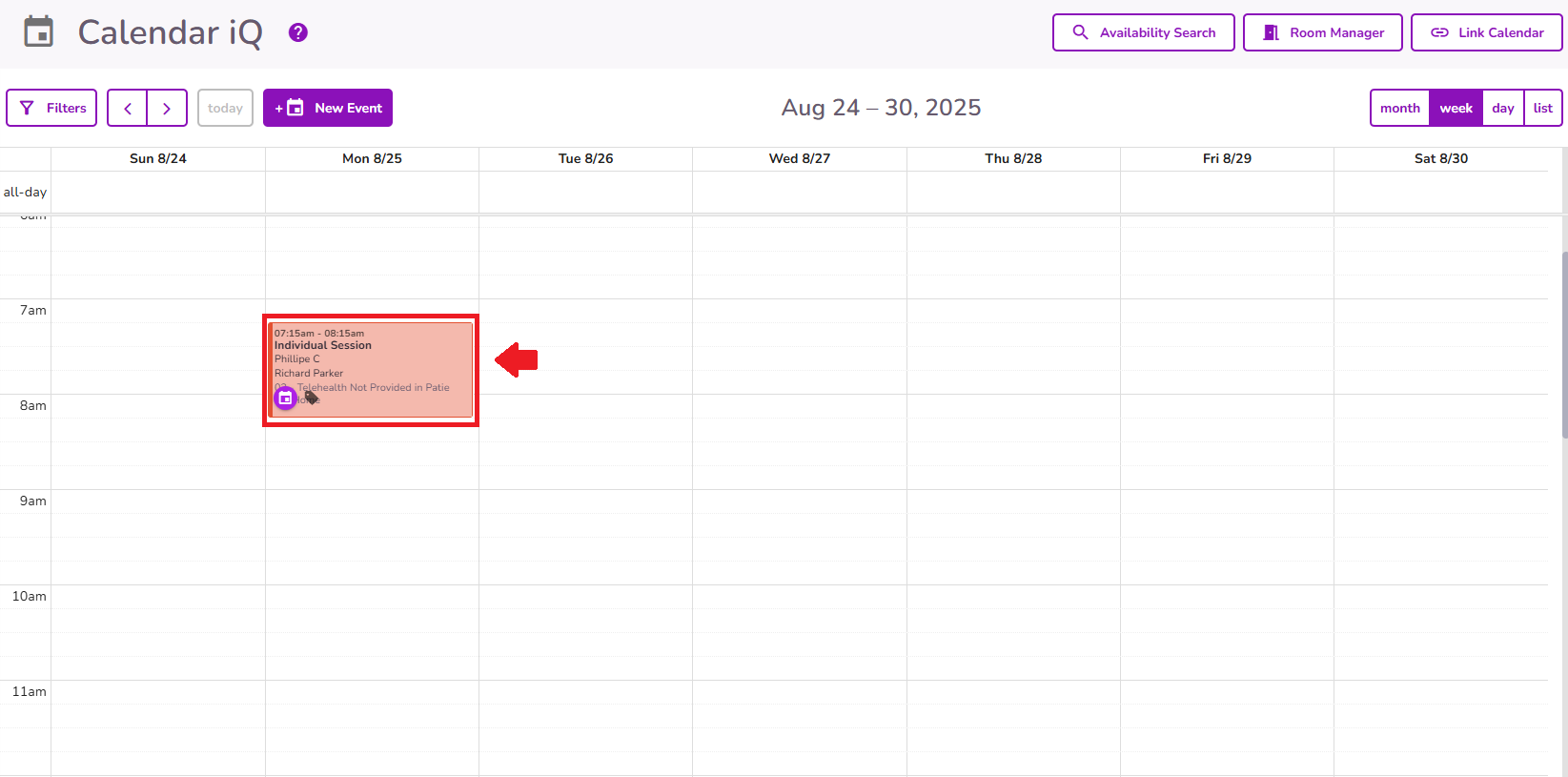
From the navigation bar select Calendar iQ

Once on the Calendar, select the appointment needing a Progress Note
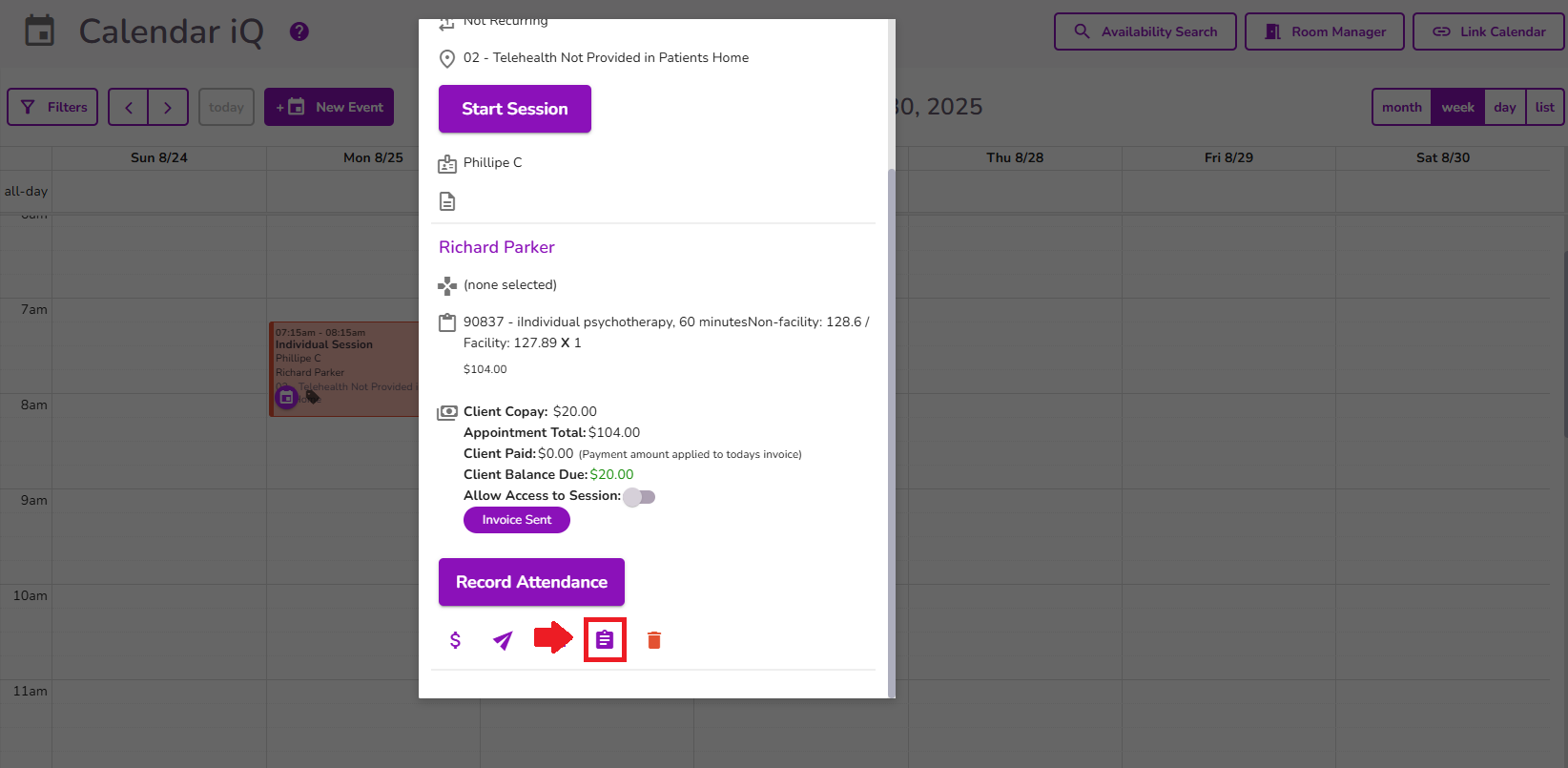
Select the Documentation icon from the event pop-up
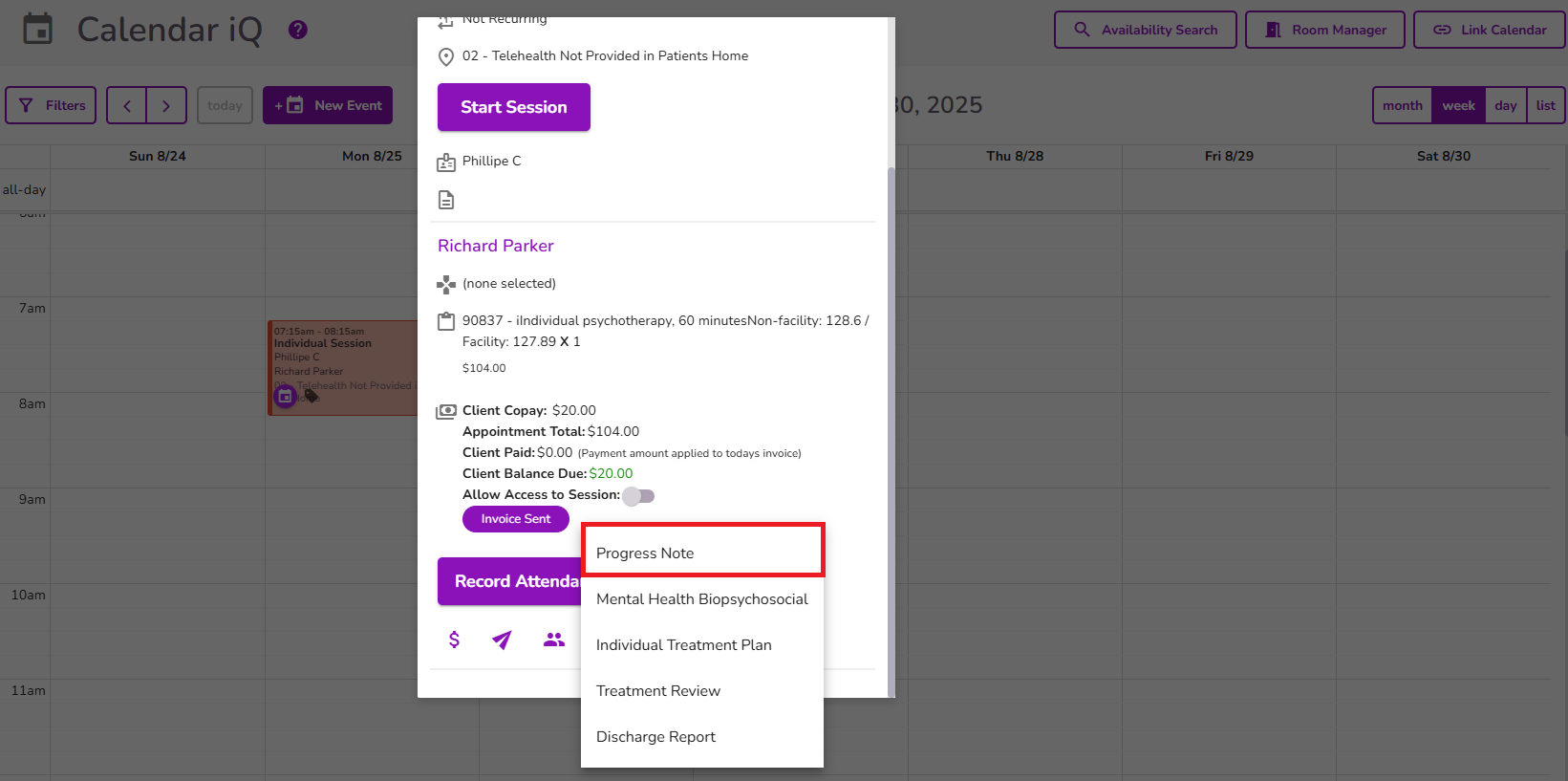
From the menu, Select Progress Note
The Session Progress Note form will appear
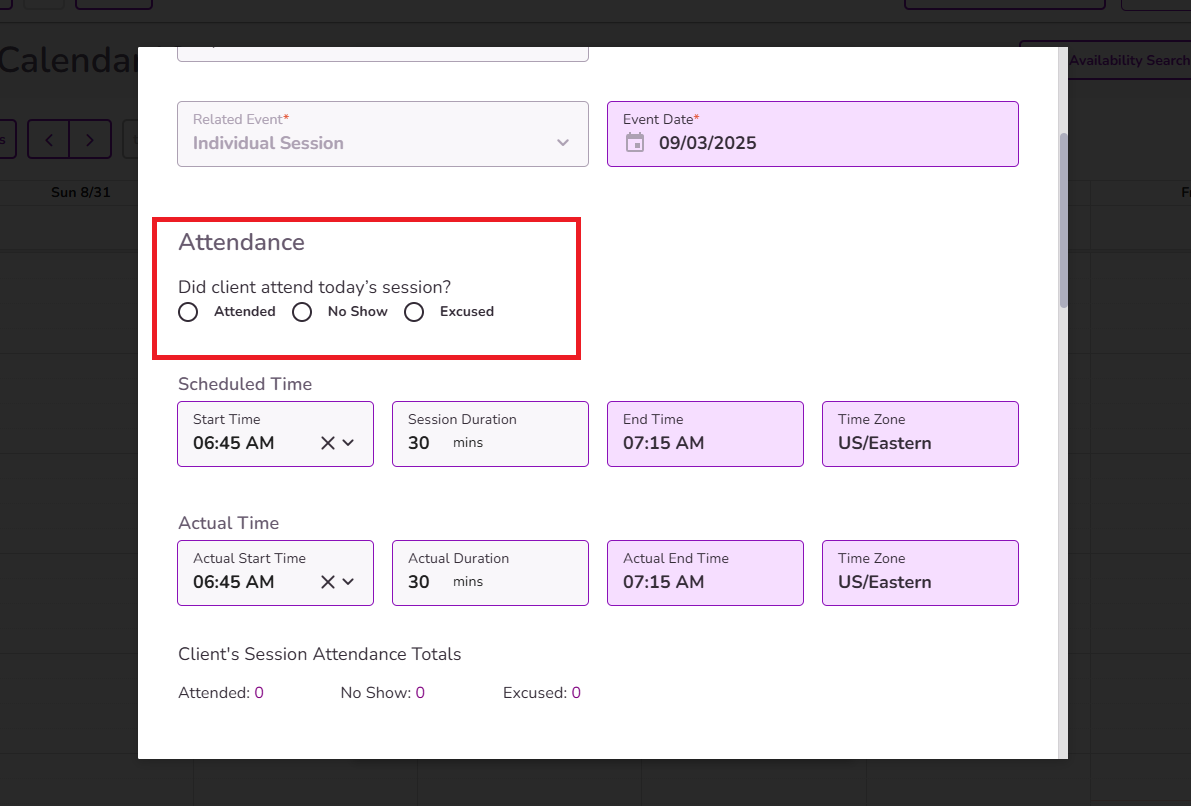
NOTE: TiQ will automatically generate the Client Name, Related Event, Date, Progress Note Type, Scheduled and Actual Start Time, End Time, and Session Duration.
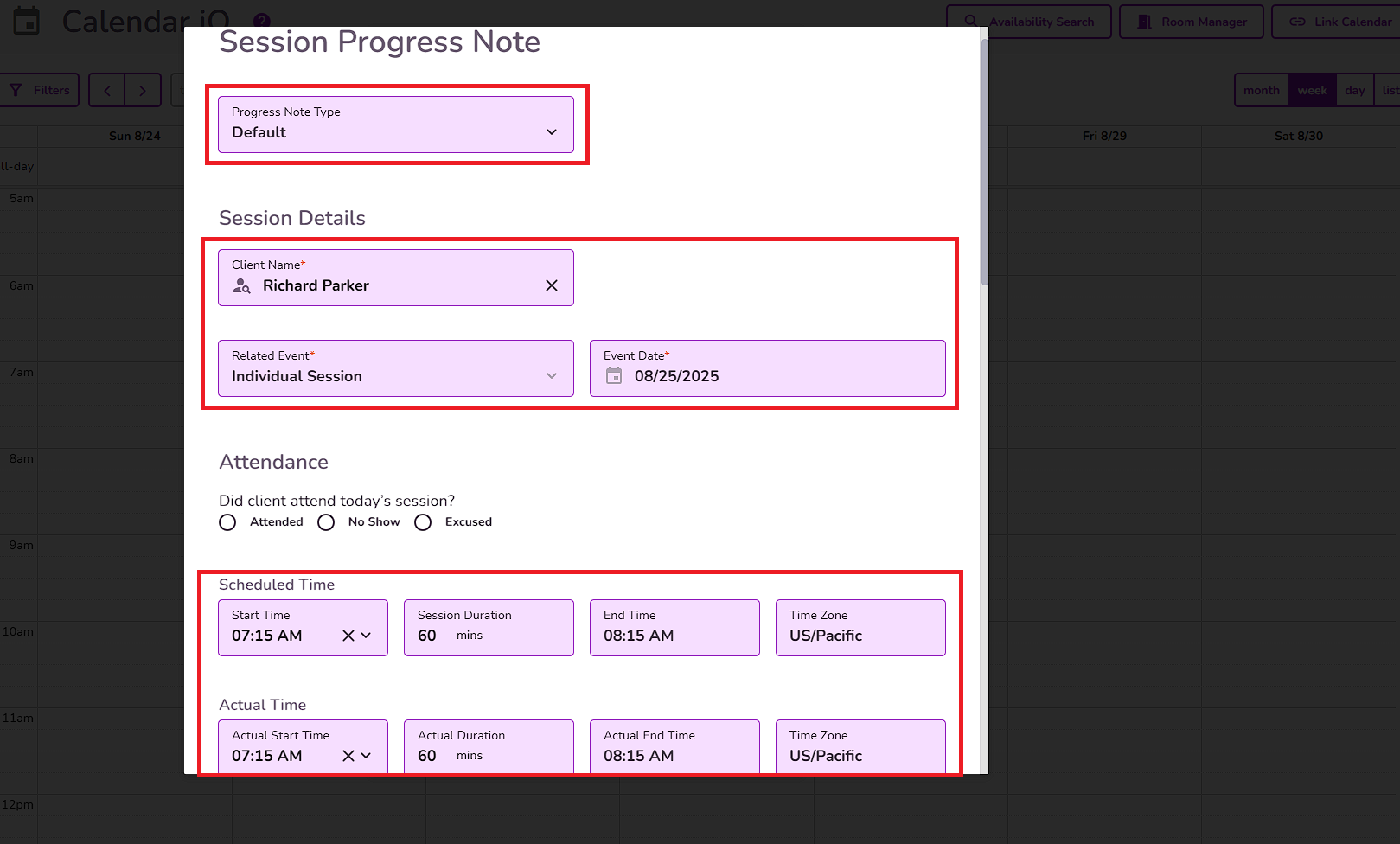
Session Attendance Totals will show a count of attended sessions, no-shows, and excused absences
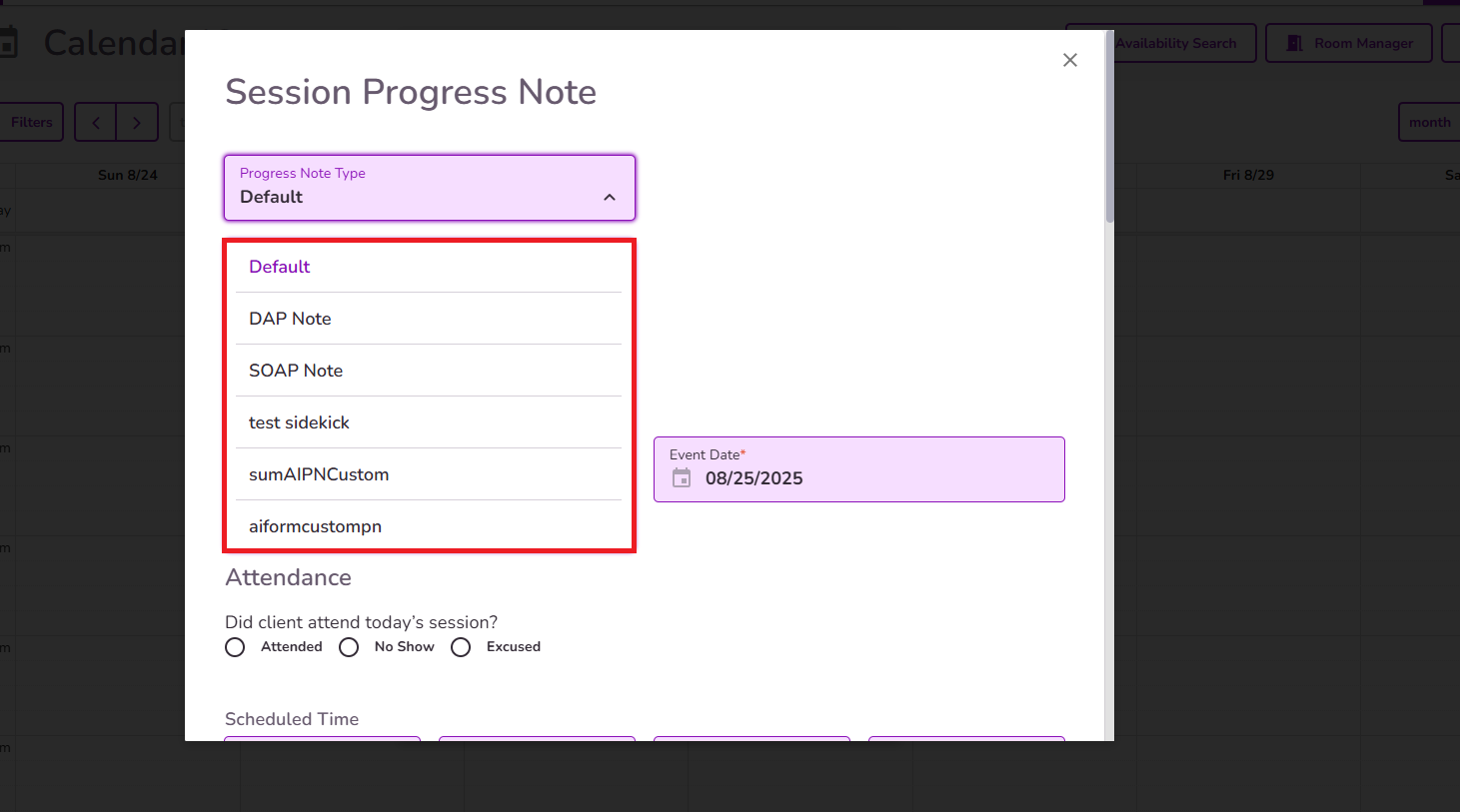
NOTE: The Form Type will be pulled from the ‘Choose default progress note type’ in the Practice Manager Settings. This settings will display the options Default, DAP note, SOAP note, and any custom progress note types from the practice.

Selecting a progress note type from the ‘Choose default progress note type’ dropdown field sets the ‘Form Type’ field in the progress note to the chosen type by default.
Users can still change or select any other option from the ‘Form Type’ field when creating a progress note.
Important: When completing a Progress Note using the same note type from a previous note, the "Auto Fill Previous Note" button will appear.
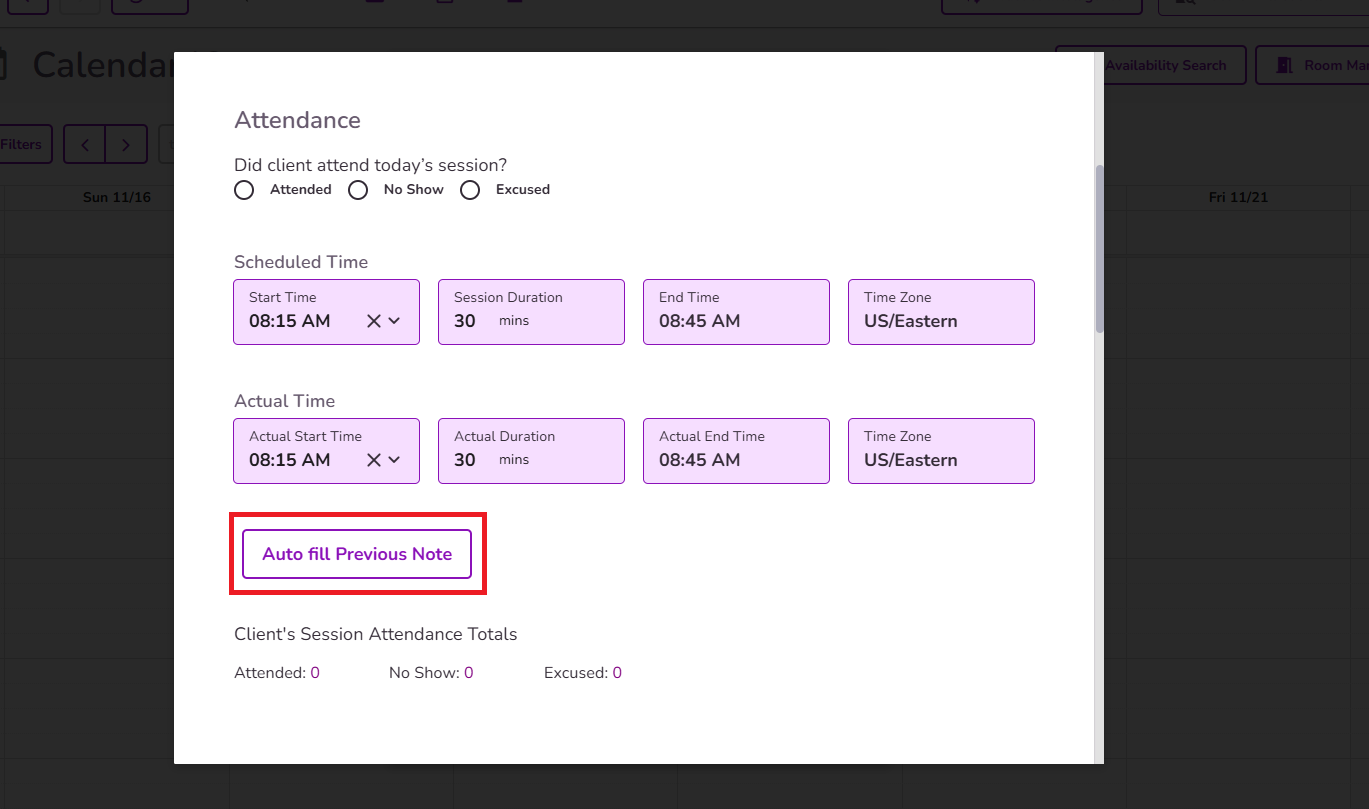
When selected, it will pull the information from the most recent note of that same type into the current note. This allows users to automatically carry over relevant clinical details and treatment plan goals into the new note based on the selected type.
Select the attendance status and verify that all other event details are accurate. You can add multiple services and staff members if needed.
NOTE: Session attendance totals will be shown for easy tracking and a quick overview of the attendance history.
Diagnosis codes added to the client's profile or treatment plan will be available for selection within the progress note. You can manually choose any or all of them, making it easy to track and reference their diagnoses.
NOTE: These codes will also appear in the PDF version of the note for clear documentation.

Medications information is available within the Progress Note and displays medication data retrieved directly from Dr. First. All medication information shown is read-only and reflects the most current data available from Dr. First at the time the note is created.
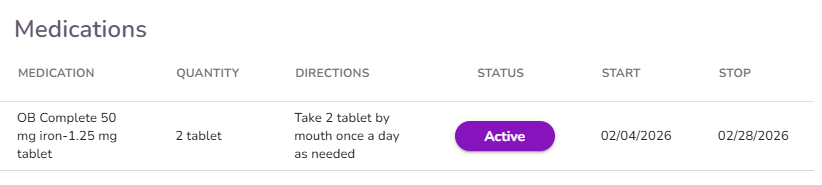
IMPORTANT: The medications visible in the progress note are only the ones that were prescribed through that document. If you'd like to review the full list of medications, regardless of when they were prescribe, you'll need to navigate to RCopia or to the Clinical Info tab in the client profile.
NOTE: The Medications table is available on the Client Profile for all providers. However, within the Progress Note, the Medications table is only visible to providers who have access to the ePrescribe feature.
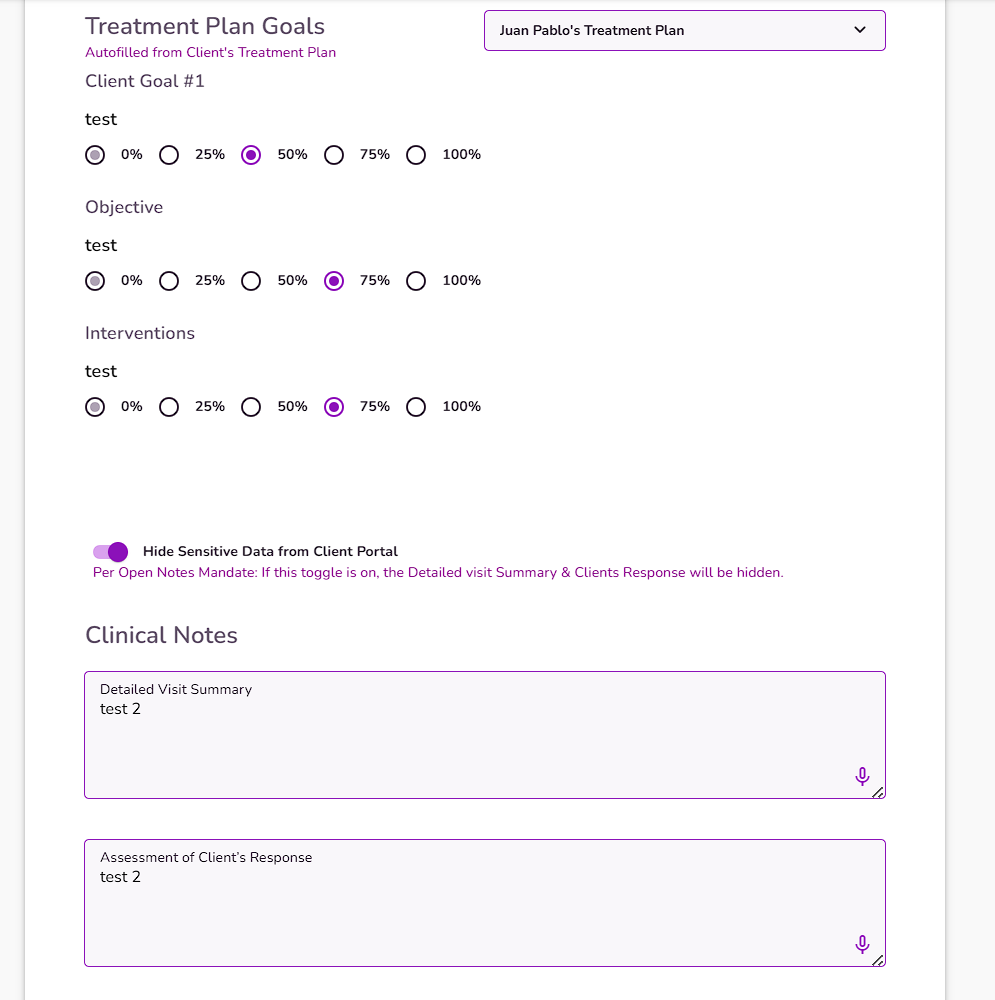
In the Treatment Plan Goals section, select a Treatment Plan from the dropdown. TiQ will automatically generate the client's treatment goals, objectives, and interventions from the selected client’s treatment plan.

Use the radial percentage selectors next to each Goal, Objective, and Intervention to indicate progress:

Available percentages: 0%, 25%, 50%, 75%, and 100%.
Click once to select a percentage. The value will auto-save.
NOTE: The last selected percentage will remain visible in default state for future reference.

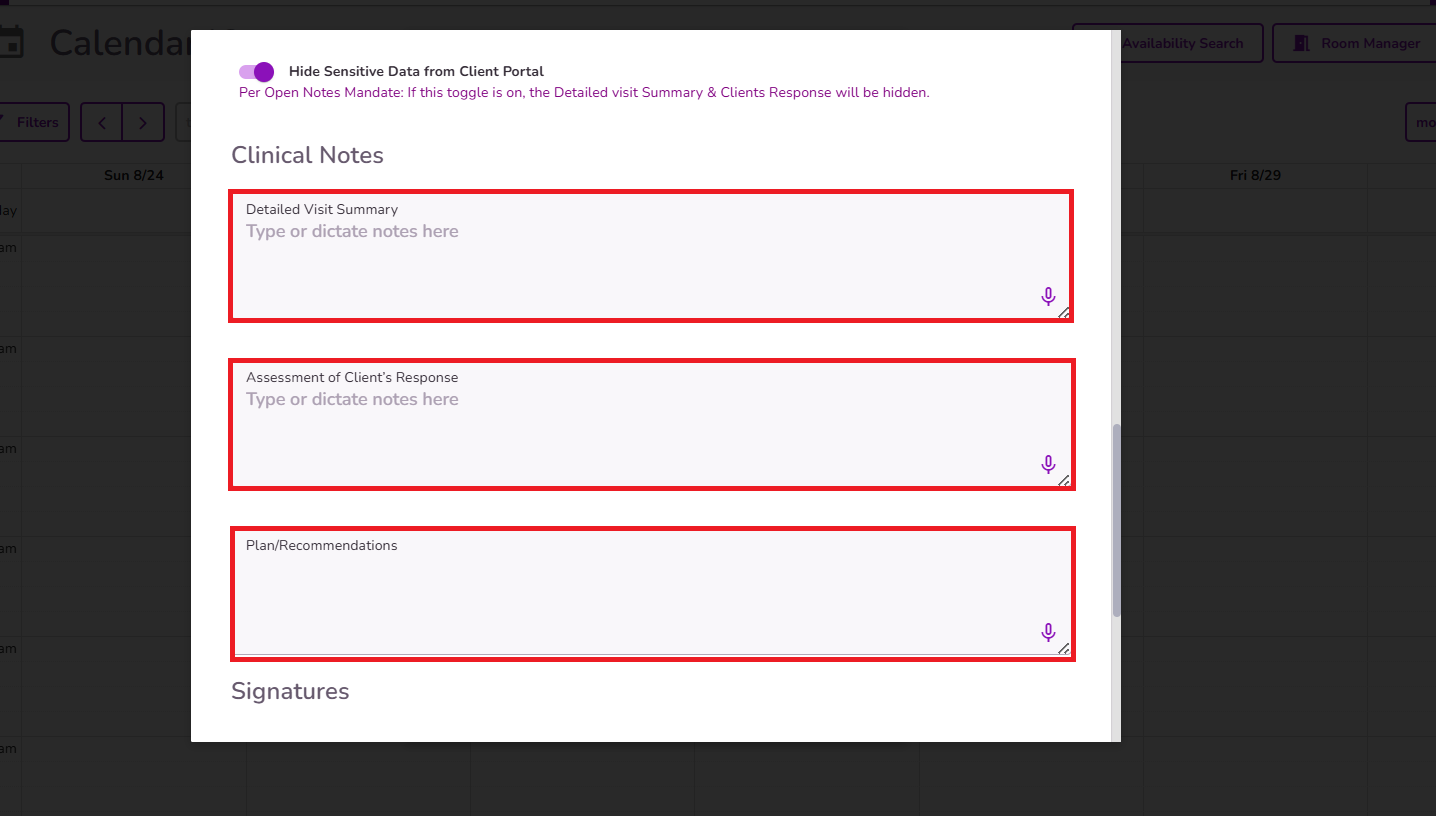
Complete Detailed Visit Summary, Assessment of Client Response and Plan/Recommendations
NOTE: The notes left in the last progress note completed will populate into the new progress note, you can use this data for reference when completing the most current progress note
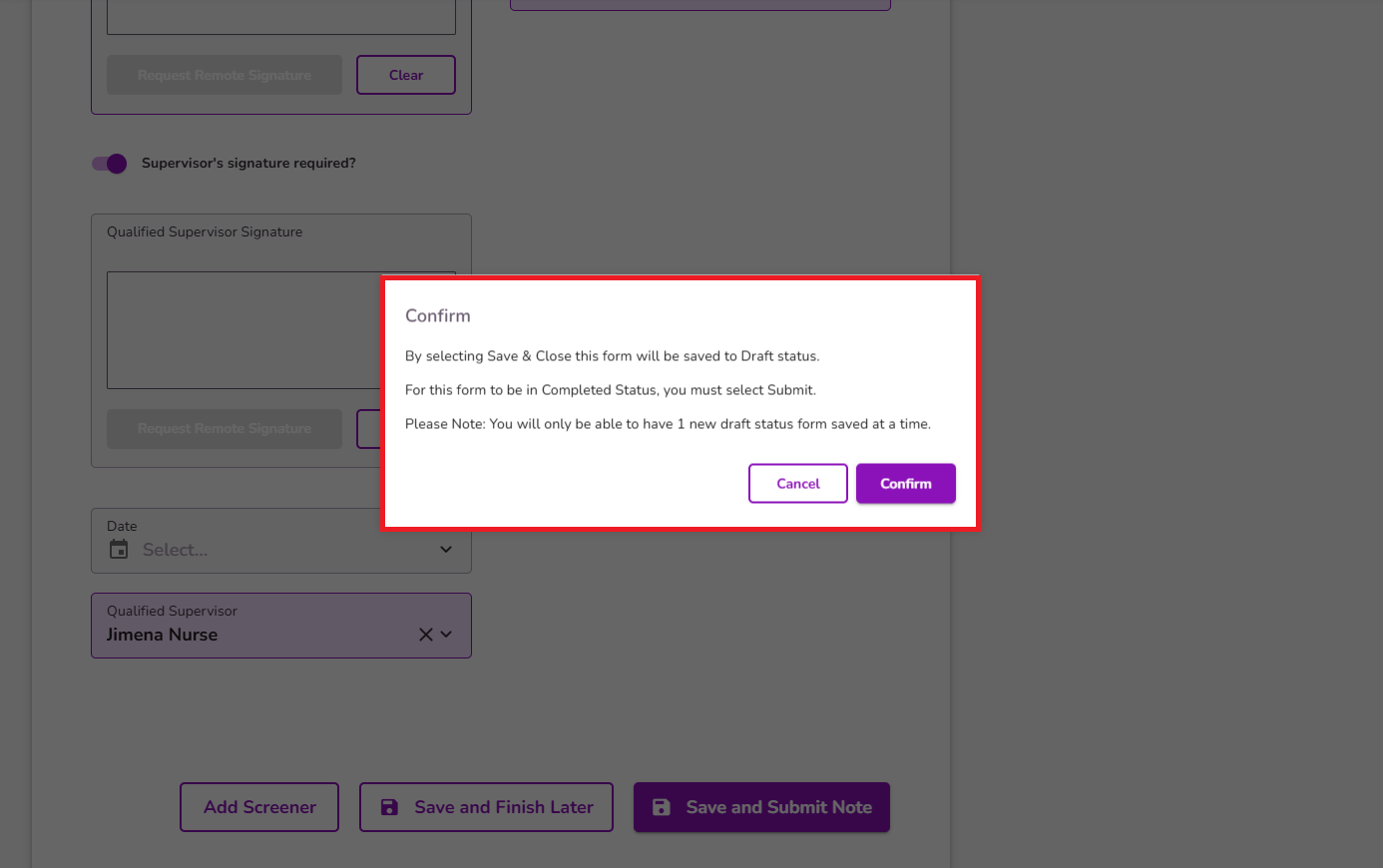
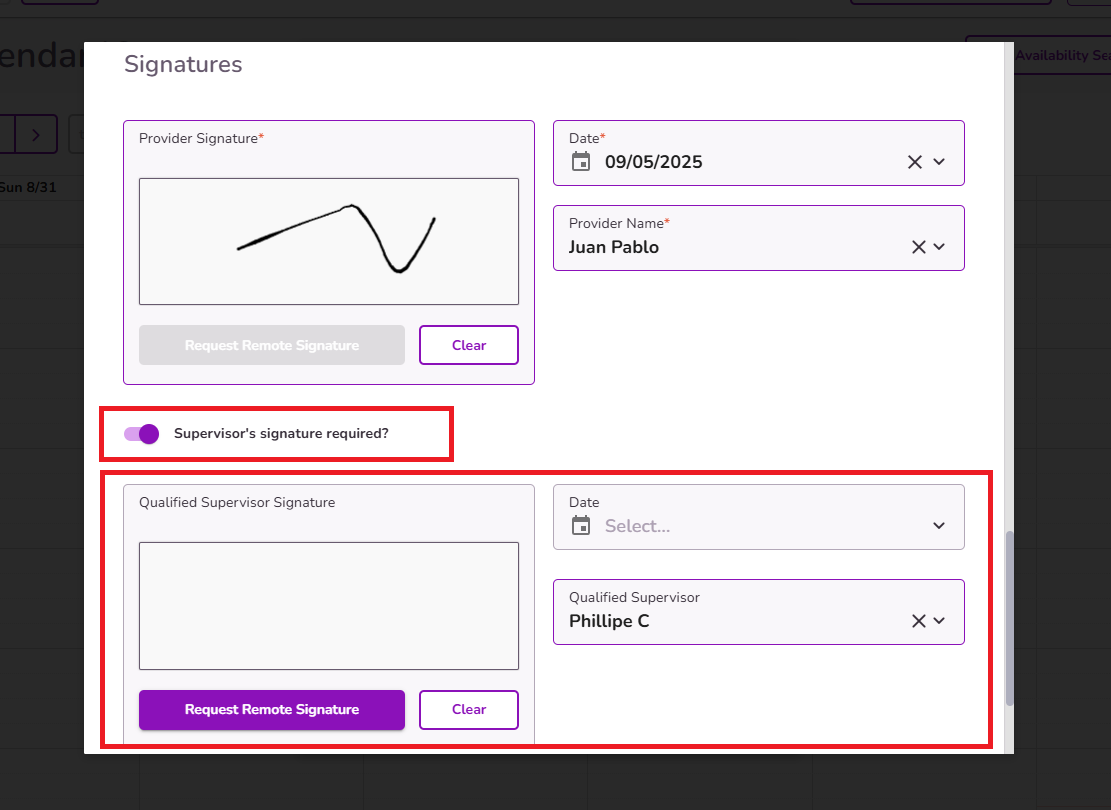
If you need the supervisor to review and sign the note, be sure to enable the Supervisor’s Signature Required? toggle. Once the note is submitted, an alert will be generated for the supervisor, prompting them to review and sign it from their end.
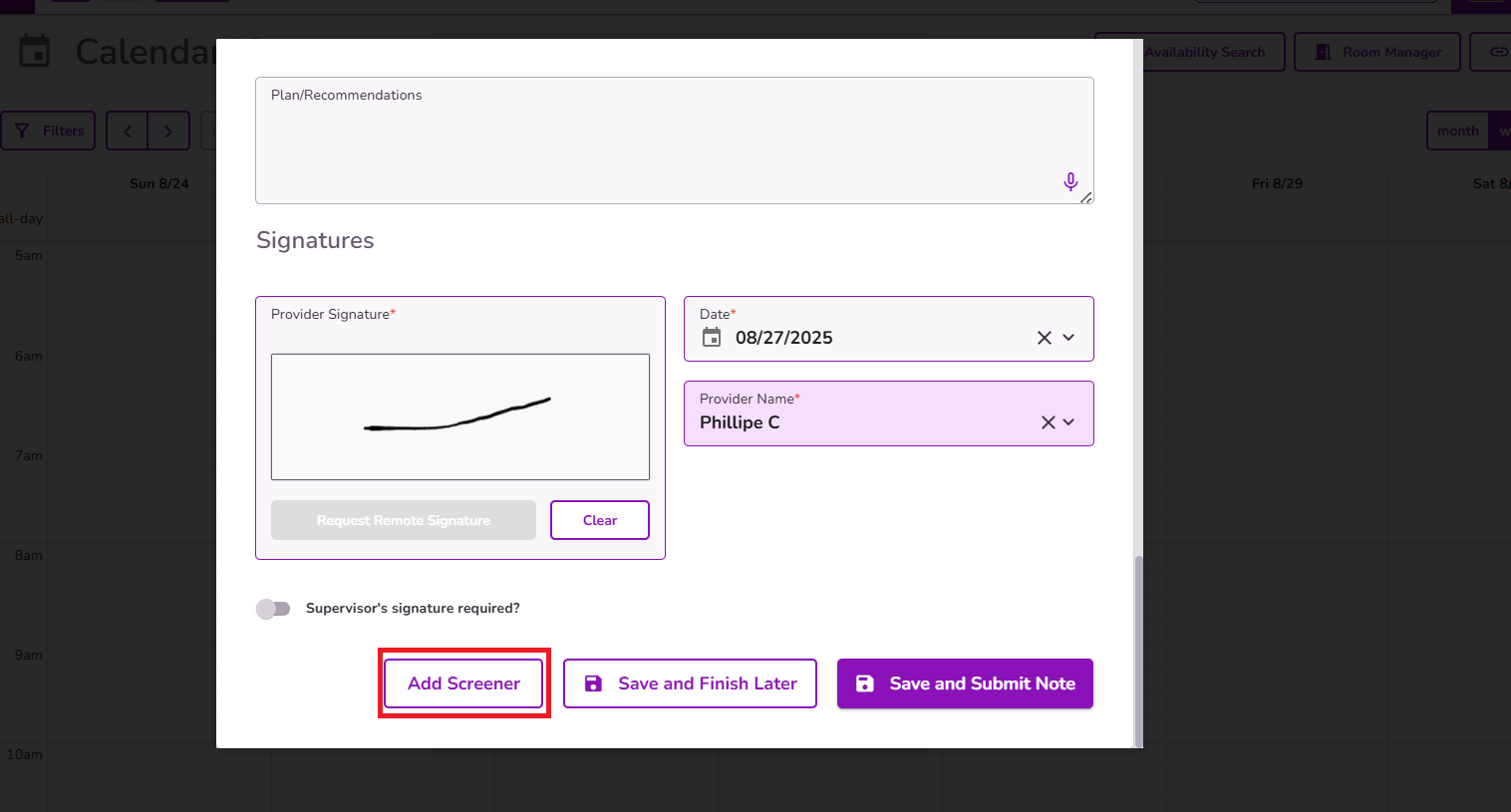
From the progress note, you have the option to complete a screener if needed. Once submitted, the screener will be automatically saved in the Forms Library and in Client Files within the client’s profile.
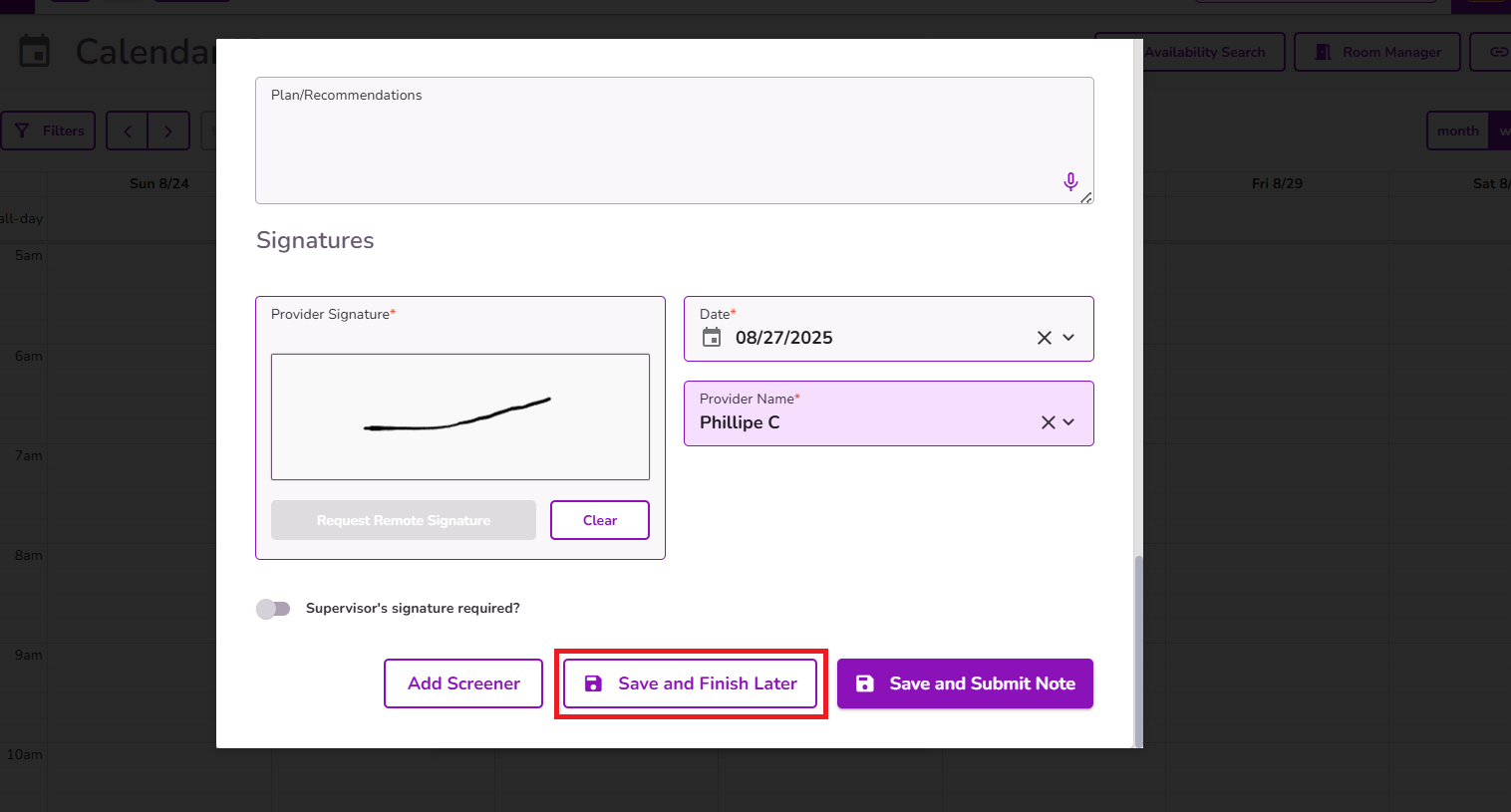
You can select Save and Finish Later to save the progress note as a draft in the client’s profile. Please note that only one draft is allowed per documentation type, meaning the system will prompt you to complete the existing draft before creating a new progress note.
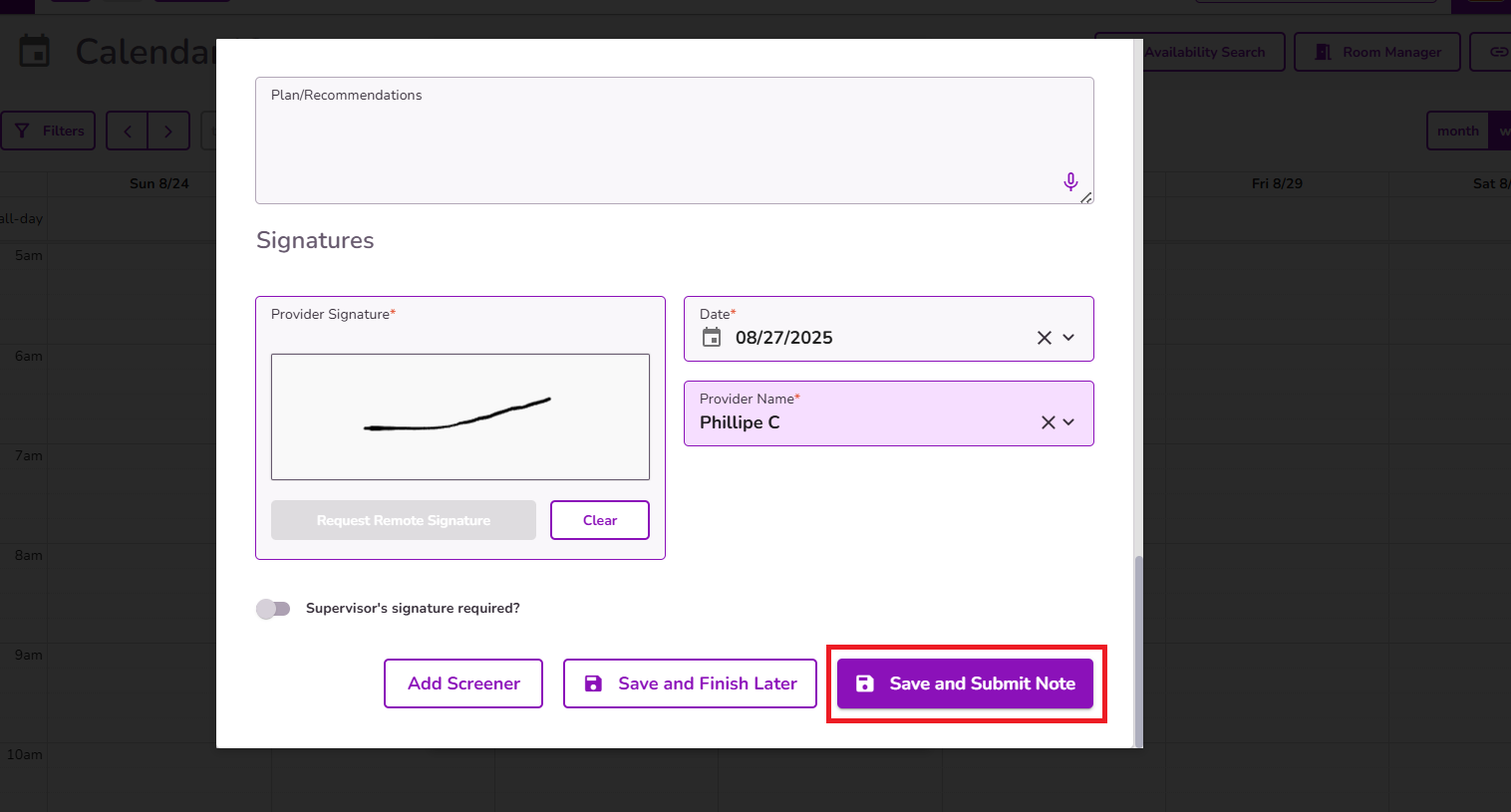
Once the Progress note is completed select Save and Submit Note to properly submit the note.
IMPORTANT: The system allows saving one draft per provider, note type, and client combination. This means that a single provider can have multiple drafts saved at the same time for different note types, and multiple providers can also have separate drafts saved for the same client at the same time.